|
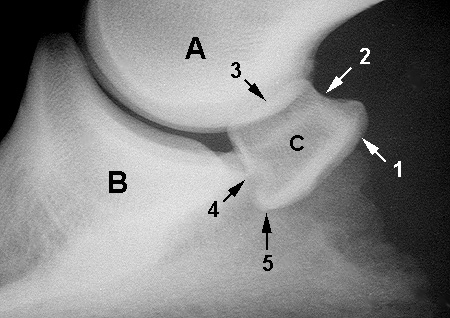
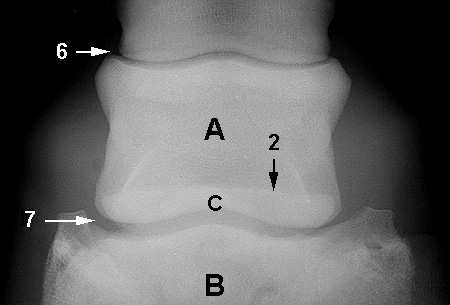
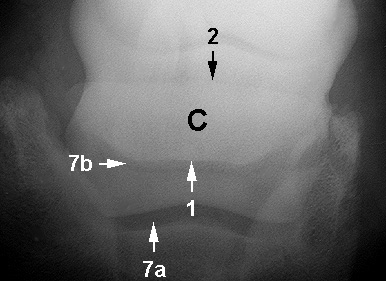
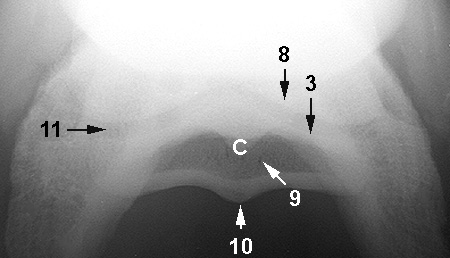
A - Middle phalanx
B - Distal phalanx C - Navicular bone 1 - Flexor cortex 2 - Proximal border 3 - Articular surface 4 - Distal border 5 - Ridge to which impar ligament attaches 6 - Proximal interphalangeal joint 7 - Distal interphalangeal joint a - Palmar aspect b - Dorsal aspect 8 - Palmar aspect of middle phalanx 9 - Nutrient foramina 10 - Sagittal ridge 11 - Articulation between navicular bone and middle phalanx |
|
Navicular syndrome is not a typical disease. There are no (public) records of racehorses that have suffered this traumatic disease, although it is supposedly fairly common (Landers, 2011). The “initiating cause and pathogenesis of navicular bone degeneration is not understood” (Sampson et al., 2009). It is thought that “pathologic changes in the flexor surface of the navicular bone play a role in the development of navicular syndrome. Initially, degeneration of the fibrocartilage of the flexor surface is thought to develop as a result of supraphysiologic [greater than normal] loading (Widmer et al., 2005). Most research points to the general idea of necrosis, caused by either the hardening of blood vessels or a blood clot which both prevent proper blood flow to the navicular bone (Sampson et al., 2009). This causes the degeneration of the navicular bone, which is extremely painful and will naturally result in severe lameness. Trauma can also be an explanation for the development of this problem (Widmer et al., 2005), but more research must be conducted to determine the physiological reason for the degeneration seen. Diagnosis is perhaps the most beneficial thing a horse owner or trainer should do when there are signs of navicular syndrome, the biggest being extreme heel pain. According to one study involving 72 horses with signs of navicular syndrome, “The abnormalities seen on the MR images were not visible on radiographs, even though the majority of horses had changes involving the navicular bone” (Sampson et al., 2009). Another study found bone remodeling that was detectable on radiographs, but only one horse was studied (Widmer et al., 2005). These studies indicate that some navicular changes can be detected with radiographs, but often Magnetic Resonance Imaging will be the only way to diagnose the problem completely. “Deep digital flexor tendonitis was recognized previously in horses with adhesion of the tendon to the navicular bones […] and has been recognized as a primary problem in some horses with clinical signs of navicular syndrome” (Sampson et al., 2009). The link between this inflammation and the necrosis of the navicular bone is currently unknown. Thirteen of the 72 horses from the first study were diagnosed with deep digital flexor tendonitis (Sampson et al., 2009). The MRI’s from the study also did not support the idea of “increased synovial fluid in the navicular bursa as a primary entity” of the problem (Sampson et al., 2009). The microscopic findings in the study of the individual horse indicated “an increased number of trabeculae in the medullary cavity [central cavity], a cyst in the sagittal ridge of the flexor cortex [palmer side] and large synovial fossae that extended from the distal border into the medullary cavity” (Widmer et al., 2005). The researchers also found that “MR imaging was most useful for identifying soft tissue changes of the navicular region. The superior contrast afforded by MR imaging is indispensable for recognizing pathologic changes in tendons, ligaments, cartilage, bursae, and trabecular bone” (Widmer et al., 2005).
Treatments can include “controlled exercise, corrective shoeing, various medical and surgical treatments, and acupuncture, […] but the therapeutic benefits have been inconsistent (Schoonover, Jann, and Blaik, 2005). Corrective shoeing is based on the idea of elevating the heel to relieve strain on the Deep Digital Flexor Tendon, thus relieving some of the pain around the navicular bone. Nonsteroidal anti-inflammatory derivatives are commonly used to keep the horse comfortable and minimize pain. In the study “Quantitative comparison of three commonly used treatments for navicular syndrome in horses,” “The addition of phenylbutazone administration to the described method of shoeing further improved the mean %BWF [percentage body weight of force applied to lame legs] of 8 [out of 12] horses” (Schoonover, Jann, and Blaik, 2005). Joint injections of corticosteroids have some success, but research has indicated that “Administration of hyaluronate in combination with corticosteroids has been shown to be more beneficial for the treatment of joint disease than administration of corticosteroids alone” (Schoonover, Jann, and Blaik, 2005). In severe cases a neurectomy, or “nerving”, can be performed. In a retrospective study of 57 horses, all suffering from navicular syndrome, the results were as follows: “Thirty-seven of 50 horses (74%) were sound at 1 year, whereas 29 of 46 horses (63%) were sound at 2 years. One horse […] was euthanatized because of a complication associated with the neurectomy procedure. […] 22% [of the owners] were disappointed with the long-term results” (Jackman et al., 1993). Nerving is not a long-term treatment, with the procedure often needing to be repeated when the horse begins to develop more pain and lameness.
Prevention of this problem is not always possible, as the true cause of navicular syndrome is unknown. Proper foot care is always recommended. “Long toes, underrun heels, and hoof imbalance can put excess strain on the navicular apparatus,” so a farrier must be cautious that these issues are avoided (Schoonover, Jann, and Blaik, 2005).
Treatments can include “controlled exercise, corrective shoeing, various medical and surgical treatments, and acupuncture, […] but the therapeutic benefits have been inconsistent (Schoonover, Jann, and Blaik, 2005). Corrective shoeing is based on the idea of elevating the heel to relieve strain on the Deep Digital Flexor Tendon, thus relieving some of the pain around the navicular bone. Nonsteroidal anti-inflammatory derivatives are commonly used to keep the horse comfortable and minimize pain. In the study “Quantitative comparison of three commonly used treatments for navicular syndrome in horses,” “The addition of phenylbutazone administration to the described method of shoeing further improved the mean %BWF [percentage body weight of force applied to lame legs] of 8 [out of 12] horses” (Schoonover, Jann, and Blaik, 2005). Joint injections of corticosteroids have some success, but research has indicated that “Administration of hyaluronate in combination with corticosteroids has been shown to be more beneficial for the treatment of joint disease than administration of corticosteroids alone” (Schoonover, Jann, and Blaik, 2005). In severe cases a neurectomy, or “nerving”, can be performed. In a retrospective study of 57 horses, all suffering from navicular syndrome, the results were as follows: “Thirty-seven of 50 horses (74%) were sound at 1 year, whereas 29 of 46 horses (63%) were sound at 2 years. One horse […] was euthanatized because of a complication associated with the neurectomy procedure. […] 22% [of the owners] were disappointed with the long-term results” (Jackman et al., 1993). Nerving is not a long-term treatment, with the procedure often needing to be repeated when the horse begins to develop more pain and lameness.
Prevention of this problem is not always possible, as the true cause of navicular syndrome is unknown. Proper foot care is always recommended. “Long toes, underrun heels, and hoof imbalance can put excess strain on the navicular apparatus,” so a farrier must be cautious that these issues are avoided (Schoonover, Jann, and Blaik, 2005).
